I was cardioverted on Wednesday the 28th of November. It was supposed to take an hour to an hour and a half, but took more like 4 hours, though the actual cardioversion bit was only a few minutes. For a while I no longer experienced persistent atrial flutter or any atrial fibrillation (though I know this only by looking — frequently — at a pulse oximeter, not from monitoring my perceptions of my body, which has never once spoken to me about irregularities in my heartbeat).
From the Merriam-Webster Medical Dictionary:
verb cardiovert: to subject to cardioversion // cardioverted the patient to sinus rhythm
noun cardioversion: application of an electric shock in order to restore normal heartbeat
(A kind of cousin to the defibrillation you have become accustomed to seeing on tv medical dramas.)
Advance warning: if at any point in this posting, you feel the urge to suggest a line of medical diagnosis or to offer me advice about what I should be doing, stifle that urge. If you give in to it (despite your ignorance of a grotesquely complex medical history, some of it stretching back over 50 years), you will be introducing entirely unwelcome complications into a life that has been largely devoted to medical matters for many months now, matters that are driving me frequently to despair. You will be saying, forget about coping with things, listen to my ideas and respond to me; you will become another part of the problem.
I am not asking for help. I am not asking for advice. I am offering some explanation for my frequent inattention to this blog. And I’m telling you my story, for whatever use you can make of it for yourself. I’m also complaining, in the belief that complaining for its own sake, especially to people who are in no way responsible for caring for you, can be therapeutic. A sympathetic murmur is the most such complaints should elicit.
From the Mayo Clinic site about the procedure in general:
Cardioversion is a medical procedure that restores a normal heart rhythm in people with certain types of abnormal heartbeats (arrhythmias). [I had frequent, huge spikes in heart rate — atrial fibrillation — to 160 or more beats per minute; plus an atrial flutter. The atrial fibrillation appeared quite suddenly (I had been getting pulse rate checks three or more times a week for a couple of years, without any irregularities. And then suddenly, zap. I was immediately put on a blood thinner — Eliquis — which I will need to take for the rest of my life.) These very frequent alarming events were completely undetectable by me (except by taking my pulse).]
Cardioversion is usually done by sending electric shocks to your heart through electrodes placed on your chest. It’s also possible to do cardioversion with medications.
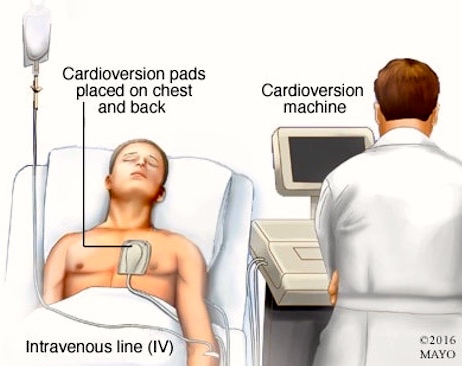
(#1) The set-up for my cardioversion. Mild burning on the chest is common.Cardioversion is usually a scheduled procedure that’s performed in a hospital. [They used a recovery room rather than an operating room.] You should be able to go home the same day as your procedure. [They kept me around for a couple of hours to watch how things developed. They provided an astonishingly tasteless hospital lunch (to compensate for my having fasted for 16 or so hours before the procedure).] For most people, cardioversion quickly restores a normal heart rhythm. [As it did in my case, after just one jolt.]
Why it’s done: Cardioversion can correct a heartbeat that’s too fast (tachycardia) or irregular (fibrillation). Cardioversion is usually used to treat people who have atrial fibrillation or atrial flutter. These conditions occur when the electrical signals that normally make your heart beat at a regular rate don’t travel properly through the upper chambers of your heart.
Cardioversion is performed when your heart is beating ineffectively. It’s usually scheduled in advance but is sometimes also done in emergency situations.
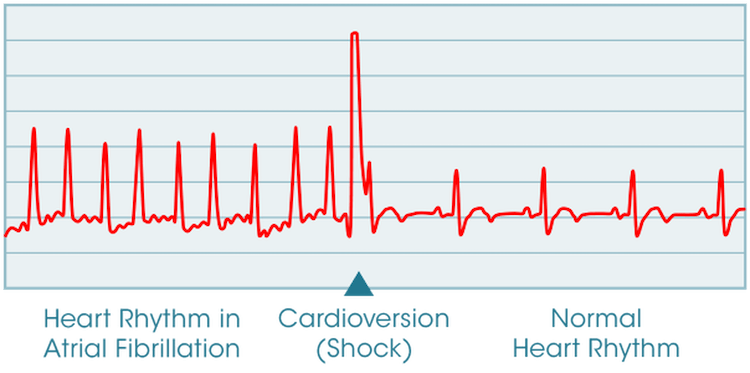
(#2) A typical graph of heart rhythm during cardioversion
About ten days after the procedure I went in for an EKG to check on the state of my heartbeat. Mixed news.
The good news is that the a-fib spikes were gone — not a surprise to me, since I’d been neurotically checking my pulse rate many times a day. The bad news is that the flutter had returned. I’ll see one of my cardiologists next week to evaluate what to do about the flutter; the likelihood is that he’ll just suggest living with it, since it’s unlikely to be life-threatening. We’ll see.
The a-fib is one of my three medical mysteries — the mystery in this case being why it suddenly appeared.
The second mystery is a form of incapacitating muscle pain (with terrible cramps), associated with a notable increase in the levels of the enzyme creatinine kinase in my blood; the ultimate cause appears to be some autoimmune condition, but tests haven’t pinned it down. It appeared independently of the other two medical mysteries, and has been controlled symptomatically by the drug prednisone (with an assortment of unpleasant side effects of its own).
The third, and by far most important, mystery is a grave shortness of breath on certain kinds of exertion — a condition that limits how far I can walk from my house. It appeared suddenly during an extreme heat wave several years ago and has frustrated a huge assortment of specialists. All their hypotheses have led nowhere. Attempts at getting a 10 to 15 percent improvement on several different fronts, in the hope that they’d add up to a signficant improvement, have had very modest success. I’m using a CPAP machine for sleep apnea, for instance; objectively, it’s clear that my number of apnea events has decreased quite a lot — but without any subjective improvement at all, and without any effect on the dyspnea. Controlling the a-fib has objectively improved my heart function, but again without any subjectve improvement at all, and without any effect on the dyspnea. And so on, though a long list of treatments and practices.
This is where I exhort you, passionately, not to engage in speculative diagnosis or offer advice from your reading or your own experiences. That will only make my life more complex, and I will tell you to go to hell (and, if you cannot resist the impulse, to get out of my life entirely).
More recently, I’ve had a cascade of dreadful medical events that started (early in the new year) with the world’s worst sinus infection: oceans of gross mucus, endless hacking, exhaustion, splitting sinus headache, and anosmia (loss of my sense of smell, hence most of my sense of taste). This was followed by sudden lightning strikes of osteoartrithis pain all over my body — paralyzing pain in my left knee, then in many other joints (“pseudogout”, caused by spiky crystals in the joints) — and by the potentially life-threatening skin infection cellulitis in my lower left leg and by edema in both legs and feet. All except the last have passed away under treatment, and I’ve had an ultrasound that showed no blood clots in my legs; more doctoring to come next week.
Working my way back to the ordinary mystery ailments. Each day a bit better on that route.
January 24, 2019 at 1:58 pm |
Complaining–at great length, in exquisite detail, and to all who have the capacity to listen in sympathetic silence–is absolutely therapeutic, and quite possibly healing.
It’s a Law of Nature.
January 24, 2019 at 5:48 pm |
My RN husband won’t let me watch hospital dramas (‘cause he doesn’t get paid), but he tells me procedure you didn’t have is defibrillation, and doesn’t entail shin removal!
January 24, 2019 at 5:53 pm |
I caught the typo — defibulation for defibrillation — a while ago and corrected it, but I’m keeping your comment for its charm. Indeed, no fibulas were harmed in the procedure I underwent.
January 25, 2019 at 7:39 am |
Although the term “apnea” is familiar to me because of the many people I know who have sleep apnea, the word dyspnea is new to me (although its meaning is easily derivable). I suppose one of the side effects of all this medical trauma is exposure to a lot of previously unfamiliar technical terms.
I’m sorry you’re going through all this. I hope the professionals can eventually figure it all out (and alleviate the various conditions).
January 25, 2019 at 8:02 am |
I’m just tickled by the term “dyspnea”. I note that it appears regularly in medical summaries but has never actually been pronounced in my presence by any medical staff (they all say “shortness of breath”).
The current addition to the terminology is the name for the cause of my inflammatory arthritis pain:
from the Arthritis Foundation site here:
https://www.arthritis.org/about-arthritis/types/calcium-pyrophosphate-deposition-disease-cppd/
January 27, 2019 at 8:17 am
has never actually been pronounced in my presence by any medical staff (they all say “shortness of breath”).
That makes sense; it’s a good thing for medical professionals to use terms they know their patients will recognize and understand, rather than intimidate them with jargon.